 What Research Shows
What Research Shows
QUICK ANSWER
| Yes — strength training is safe for most people with POTS when properly structured and supervised. Research consistently shows that a progressive, individualized resistance and aerobic training program can significantly reduce POTS symptoms, improve quality of life, and in some cases lead to full clinical remission. The key is starting smart: beginning with recumbent or horizontal exercise, progressing gradually, and working with a knowledgeable trainer who understands your condition. |
What Is POTS, and Why Does Exercise Feel So Hard?
Postural Orthostatic Tachycardia Syndrome (POTS) is a condition that affects the autonomic nervous system — the part of your nervous system that regulates involuntary functions like heart rate and blood pressure. When someone with POTS stands up, blood pools in the lower body, causing the heart to race to compensate. The result can be debilitating.
POTS affects an estimated 1 to 3 million Americans, predominantly women between adolescence and age 50. It can be triggered by viral infections (including COVID-19), pregnancy, surgery, or trauma. Because standing up triggers symptoms, it creates a vicious cycle: people become less active, which leads to physical deconditioning, which makes POTS worse.
CLINICAL DIAGNOSTIC CRITERIA
| POTS is clinically defined by a heart rate increase of 30 bpm in adults (40 bpm in adolescents) within 10 minutes of standing, with symptoms lasting more than 3 months and no significant hypotension. |
Common POTS Symptoms
- Racing heart rate when standing
- Dizziness and lightheadedness
- Extreme fatigue
- Nausea and brain fog
- Exercise intolerance
- Sleep disturbances
⚠ IMPORTANT: Always consult your physician or cardiologist before starting any new exercise program with POTS. Every case is different, and some individuals may require medication or additional evaluation before beginning training.
What Does Research Actually Say?
The science here is encouraging. Multiple studies confirm that structured exercise — including resistance training — is one of the most effective non-drug interventions for POTS.
Key Statistics
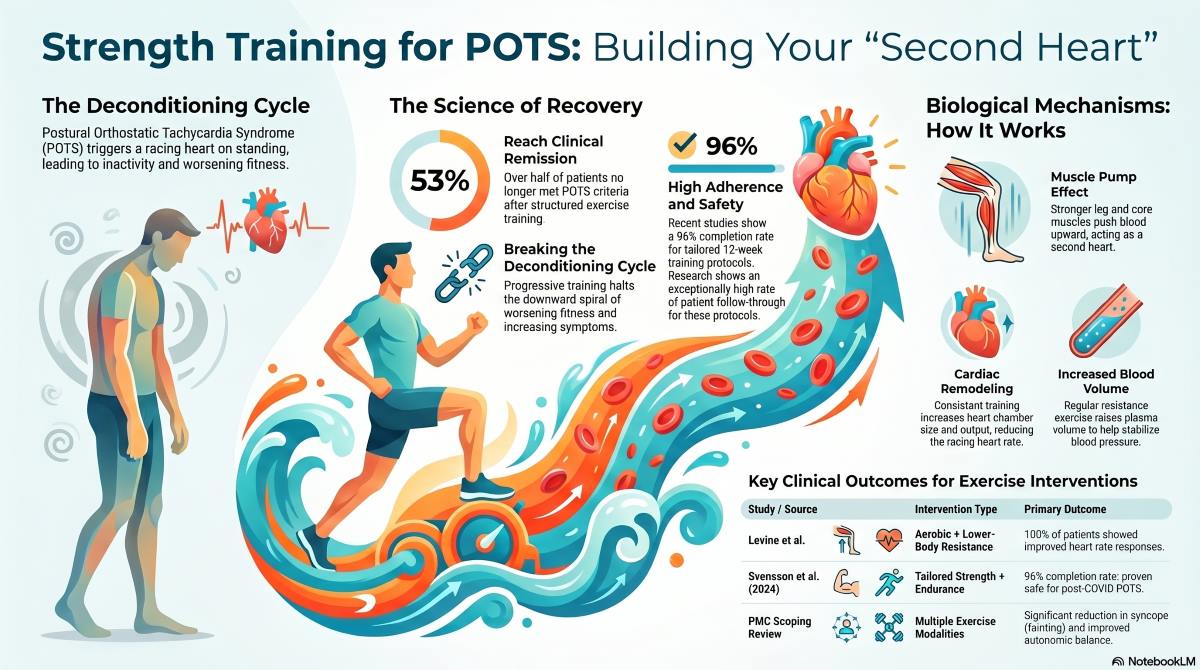
- 53% of POTS patients no longer met the clinical diagnostic criteria for POTS after an exercise program (Levine et al.)
- 96% of participants completed a 12-week tailored training protocol (Svensson et al., 2024)
A landmark study by Dr. Benjamin Levine and colleagues found that all patients who completed exercise training showed improvement in heart rate responses when standing. More strikingly, over half of participants no longer met the clinical criteria for POTS after completing the program.
A 2024 study published in Scientific Reports enrolled 26 participants with POTS (mostly women, median age 41) in a 12-week program of individually tailored endurance and strength training with weekly physiotherapist support. Nearly all participants completed the program, and the vast majority adhered to the exercise prescription.
A comprehensive 2024 scoping review analyzed multiple clinical trials and found that aerobic exercise training significantly improves symptoms for most patients with orthostatic intolerance, reduces fainting episodes, and improves both heart rate variability and cardiorespiratory endurance.
Summary of Key Research on Exercise & POTS
| Study / Source | Intervention | Key Finding |
| Levine et al. (AHA / UT Southwestern) | Structured aerobic + lower-body resistance training | 53% of patients no longer met the clinical diagnostic criteria for POTS; 100% showed heart rate improvement |
| Svensson et al., 2024 (Scientific Reports) | 12-week individualized endurance + strength training | 96% completion rate; exercise shown feasible and safe for POTS |
| PMC Scoping Review, 2024 (PubMed) | Multiple exercise modalities across clinical trials | Aerobic training significantly reduces syncope, improves autonomic balance |
| Fu & Levine (PMC) | Horizontal exercise progressing to upright training | Supervised training ‘preferable to maximize functional capacity’ |
| NIH Expert Consensus, 2019 (PubMed) | Exercise as non-pharmacological treatment | Physical reconditioning recommended as cornerstone of POTS treatment |
How Does Strength Training Actually Help POTS?
Understanding why strength training works for POTS helps explain why it needs to be done correctly. Here are the key mechanisms:
- Muscle Pump Effect: The leg and core muscles act as a “second heart,” helping push blood back up toward the heart. Stronger legs = better blood return = fewer POTS episodes.
- Increased Blood Volume: Regular exercise raises plasma and blood volume over time, which helps stabilize heart rate and blood pressure when standing.
- Cardiac Remodeling: Research shows POTS patients have smaller heart chambers. Consistent aerobic and resistance training gradually increases heart size and output, reducing the demand that causes racing heart rate.
- Improved Autonomic Regulation: Exercise training improves heart rate variability — a key marker of autonomic nervous system function — helping the body respond more appropriately to postural changes.
- Reduced Deconditioning Cycle: Breaking the cycle of inactivity is one of the most important steps. Even gentle progressive training halts the downward spiral of worsening fitness and worsening symptoms.
How Strength Training Benefits People with POTS Across Age and Gender
POTS does not affect everyone equally — age and biological sex both play a meaningful role in how the condition presents and how the body responds to training. Understanding these differences can help set realistic expectations and make your exercise program even more effective.
Adolescents and Young Adults (Ages 13–25)
POTS is most commonly diagnosed in females between the ages of 15 and 25, a period of rapid hormonal change that can affect blood volume regulation and autonomic function. For this group, strength training offers particularly powerful benefits: building lean muscle mass during these formative years improves the body’s ability to circulate blood, supports bone density, and creates a fitness foundation that can reduce symptom severity well into adulthood. Young women in this age group also tend to respond quickly to progressive training, often seeing measurable improvements in standing heart rate and daily energy levels within the first 8 to 12 weeks of a structured program. The key for adolescents is age-appropriate programming that emphasizes technique, gradual load progression, and adequate recovery — never pushing for athletic performance at the expense of symptom management.
Women in Their 30s and 40s
For women in their 30s and 40s — who represent the largest segment of adults living with POTS — strength training addresses several overlapping challenges at once. Hormonal fluctuations tied to the menstrual cycle and perimenopause can worsen POTS symptoms, particularly during the luteal phase when blood volume naturally decreases. Regular resistance training helps counteract this by improving overall circulatory efficiency, building lower-body muscle mass to enhance the venous pump, and supporting a healthier resting autonomic tone. Women in this age range who commit to consistent training also gain protective benefits beyond POTS: better bone density, improved insulin sensitivity, reduced anxiety, and greater metabolic resilience — all of which contribute to an improved quality of life when managing a chronic condition.
Men with POTS
While POTS is far more common in women, men do develop the condition. The same evidence-based principles that apply to women apply to men: progressive, individualized programming that starts in recumbent or seated positions and advances gradually as tolerance improves. Male patients should not assume that greater baseline strength means they can train harder from the start — a gradual, symptom-guided approach remains essential regardless of gender.
Older Adults (Ages 50+)
Although POTS is less commonly diagnosed after age 50, adults in this group may develop the condition following illness, surgery, or prolonged bed rest, and they face additional challenges due to age-related muscle loss (sarcopenia) and reduced cardiovascular adaptability. For older adults with POTS, strength training is especially valuable because it directly combats the muscle wasting that worsens orthostatic intolerance. Resistance exercise preserves and rebuilds the leg and core muscles that act as a natural pump for venous blood return, helping stabilize heart rate when standing. Low-impact, chair-assisted, or recumbent resistance movements are excellent entry points, with progression carefully guided by a knowledgeable trainer. The goal for this group is functional independence — improving the ability to stand, walk, and perform daily activities without triggering debilitating symptoms.
Frequently Asked Questions
Can strength training make POTS worse?
If done incorrectly — too much, too soon, in a standing position before the body is ready — exercise can temporarily worsen symptoms. However, with proper programming that starts recumbent and progresses gradually, research shows exercise is generally safe and beneficial. Minor symptom fluctuations are expected; significant worsening should be discussed with your doctor.
How long before I see improvements from training?
Most research studies use 12-week programs and report significant symptom improvement within that timeframe. Some individuals notice improved exercise tolerance within 4–6 weeks. Long-term consistency — 6 to 12 months — produces the most meaningful and lasting results.
Do I need a special trainer, or can any gym trainer help me?
Ideally, you want a certified personal trainer who is familiar with POTS and autonomic conditions. Generic programming designed for healthy adults can be counterproductive or unsafe for someone with POTS. Trainers at Redefine Fitness are experienced in working with clients who have complex health conditions, including POTS.
What about post-COVID POTS — is it different?
Post-COVID POTS is increasingly common and represents a growing segment of new diagnoses. The 2024 Svensson study specifically focused on post-COVID POTS and found individualized exercise to be both feasible and safe. Extra care around pacing strategies is recommended, as post-exertional malaise (PEM) can be a factor.
Can children and teenagers with POTS do strength training?
POTS is common in adolescents, and supervised, age-appropriate exercise is recommended. Studies in pediatric POTS populations show improvements in functioning following structured training. Always work with a pediatric cardiologist and a trainer experienced with youth fitness.
| Train Smarter with POTS — We’re Here to Help
At Redefine Fitness, our certified trainers understand the complexity of POTS and other autonomic conditions. We design individualized, progressive programs that meet you exactly where you are — safely building strength, stamina, and confidence at every step. |
Sources & References
- Svensson, A. et al. (2024). Individually tailored exercise in patients with postural orthostatic tachycardia syndrome related to post-COVID-19 condition. Scientific Reports, 14, 20017. https://doi.org/10.1038/s41598-024-71055-5
- Exercise Interventions in the Management of Postural Orthostatic Tachycardia Syndrome: A Scoping Review. (2024). PubMed Central. https://pmc.ncbi.nlm.nih.gov/articles/PMC11646465/
- Pena, C. et al. (2024). Exercise in Postural Orthostatic Tachycardia Syndrome: Focus on Individualized Exercise Approach. Journal of Clinical Medicine. https://www.mdpi.com/2077-0383/13/22/6747
- Fu, Q. & Levine, B.D. (2018). Exercise and Non-Pharmacological Treatment of POTS. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC6289756/
- Fu, Q. et al. (2011). Exercise Training Versus Propranolol in the Treatment of the Postural Orthostatic Tachycardia Syndrome. American Heart Association / ScienceDaily.
- Vernino, S. et al. (2021). Postural Orthostatic Tachycardia Syndrome (POTS): State of the Science — Part 1. PubMed. https://pubmed.ncbi.nlm.nih.gov/34144933/