| QUICK ANSWER
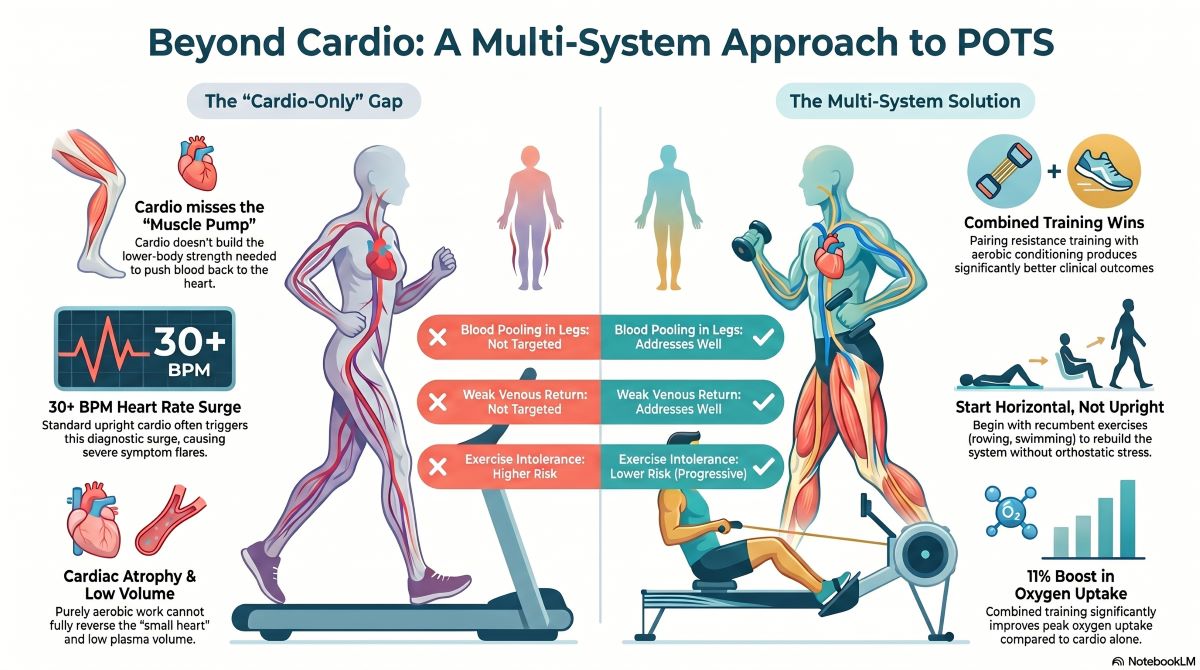
Cardio alone is not enough for POTS patients because the condition involves multiple physiological dysfunctions — including reduced blood volume, cardiac atrophy, impaired venous return, and autonomic nervous system dysregulation — that cardiovascular exercise cannot address on its own. Research shows that a comprehensive approach combining progressive aerobic conditioning with lower-body and core strength training produces significantly better outcomes than cardio in isolation. Without targeted strength work, patients remain vulnerable to orthostatic intolerance, poor circulation, and recurring symptoms even after consistent cardio efforts. |
What Is POTS, and Why Does Exercise Matter?
Postural Orthostatic Tachycardia Syndrome — or POTS — is a condition that affects the autonomic nervous system, which controls involuntary body functions like heart rate and blood pressure. When a person with POTS stands up, their heart rate shoots up rapidly (typically by 30 beats per minute or more in adults) without a corresponding drop in blood pressure. This surge can cause dizziness, extreme fatigue, brain fog, near-fainting, and nausea that make even simple daily tasks feel overwhelming.
POTS is far more common than many people realize, affecting an estimated 1 to 3 million Americans, though prevalence estimates vary depending on the source. It disproportionately affects women, with onset most commonly occurring during adolescence to early adulthood, and cases have surged following viral illnesses, including long COVID. Despite this, awareness of how to properly exercise with POTS remains limited — and many patients unknowingly make their symptoms worse by following generic cardio advice that was never designed for their condition.
| 30+
BPM heart rate increase upon standing for diagnosis |
1–3M
Estimated Americans living with POTS (range varies by source) |
11%
Improvement in peak oxygen uptake after combined training (Shibata et al., 2012) |
3–6
Months minimum for meaningful reconditioning results |
Why Cardio Alone Falls Short for POTS Patients
It’s a reasonable assumption: POTS affects the heart and circulation, so cardio should fix it. But the science tells a more complex story. POTS is not simply “being out of shape.” While cardiovascular deconditioning is a contributing factor, research published in the Journal of Clinical Medicine (2024) highlights that POTS involves multiple mechanisms — including cerebral blood flow problems, possible neuroinflammation, reduced plasma volume, and structural cardiac changes — that purely aerobic exercise cannot reverse on its own.
| KEY RESEARCH FINDING
Studies have found that neither POTS nor related conditions like ME/CFS are caused purely by deconditioning, and that exercise therapy alone is unlikely to be fully effective in improving orthostatic intolerance symptoms when applied without a comprehensive, individualized strategy. |
Here is why relying solely on cardio can be insufficient — and sometimes even counterproductive for POTS patients:
| Smaller Heart Size
POTS patients often have a physically smaller heart with reduced blood volume, leading to lower stroke volume with each beat. Upright cardio early on can worsen symptoms before improving them. |
Weak Venous Return
Blood pools in the legs when standing. Lower-body muscle strength acts as a critical pump to push blood back toward the heart — something cardio alone does not build adequately. |
| Autonomic Dysregulation
The autonomic nervous system — not just the heart — is dysregulated in POTS. Rebuilding it requires a multi-system approach including core stability, breathing work, and graded positional challenges. |
Exercise Intolerance Risk
Vigorous upright cardio can trigger severe symptom flares. Without a proper foundation first, high-intensity cardio leads to post-exertional crashes and discourages patients from continuing. |
| Low Blood Volume
Many POTS patients have reduced plasma volume — a problem cardio alone cannot fix. Combined training alongside proper hydration and sodium intake is needed to meaningfully expand blood volume. |
Neglected Core Strength
A weak core and poor postural stability worsen blood pooling in the abdomen when upright. Core and resistance training directly address these structural gaps that cardio cannot reach. |
The Crucial Role of Strength Training in POTS Management
Research consistently demonstrates that a structured program combining aerobic conditioning with resistance training produces significantly better outcomes for POTS patients than either approach alone. According to a scoping review published in PMC (2024), the most effective programs include resistance work targeting the lower body alongside cardiovascular reconditioning, beginning in recumbent or seated positions before gradually progressing to more upright postures.
Here is what strength training specifically contributes to POTS management:
- Improved venous return: Strengthening the leg muscles — especially the calves, quadriceps, and hamstrings — creates a more effective muscular pump that actively helps push blood back up toward the heart against gravity.
- Increased cardiac size and stroke volume: Combined training (cardio + resistance) has been shown to increase cardiac mass and stroke volume in POTS patients, reducing the heart’s need to compensate with a rapid rate.
- Better blood volume expansion: Exercise training combined with proper hydration and electrolyte intake helps expand plasma and blood volume, which is reduced in many POTS patients.
- Improved core stability: A strong core and abdominal muscles help regulate intra-abdominal pressure and support circulation, reducing blood pooling in the abdomen when upright.
- Enhanced autonomic control: Resistance training stimulates the baroreflex (the body’s blood pressure regulation mechanism) in ways that aerobic exercise does not, helping retrain the nervous system over time.
Cardio vs. Combined Training: What Does Each Address?
Understanding what each type of exercise targets helps clarify why a combined approach is necessary. The table below compares how cardio alone stacks up against a combined cardio + strength program across the key physiological challenges in POTS:
| POTS Challenge | Cardio Only | Combined Cardio + Strength |
| Reduced blood volume | Partial | Addresses Well |
| Small heart / low stroke volume | Partial | Addresses Well |
| Blood pooling in legs | Not Targeted | Addresses Well |
| Weak venous return pump | Not Targeted | Addresses Well |
| Core and postural instability | Not Targeted | Addresses Well |
| Autonomic nervous system retraining | Limited | Addresses Well |
| Aerobic capacity / VO₂ max | Addresses Well | Addresses Well |
| Exercise intolerance risk (early stage) | Higher Risk | Lower Risk (if progressive) |
The Importance of Starting Horizontal — Not Upright
One of the most important principles in POTS exercise is the starting position. For many patients, upright exercise initially makes symptoms worse. This is why clinical protocols developed at institutions like the Children’s Hospital of Philadelphia and UT Southwestern Medical Center begin patients in a recumbent or horizontal position before gradually advancing to more upright activities.
Types of exercise often recommended at different stages of POTS reconditioning include:
- Recumbent / horizontal phase: Recumbent bike, rowing machine, swimming, and supine floor exercises — all of which allow cardiovascular work while minimizing orthostatic stress on the system.
- Seated / semi-recumbent phase: Upright bike, seated resistance exercises, and Pilates work that builds core and leg strength while still providing postural support.
- Progressive upright phase: Gradual introduction of standing exercises, treadmill walking, and elliptical as tolerance improves — always monitoring heart rate and symptoms carefully.
| IMPORTANT NOTE
Exercise in heat is generally not recommended for POTS patients, as elevated temperatures cause blood vessels to dilate, worsening blood pooling and orthostatic intolerance. Staying cool, well-hydrated, and mindful of environment is essential during any exercise session. |
What Makes a POTS Exercise Program Effective?
Not all exercise programs are built equal — and for POTS patients, a poorly designed program can cause setbacks that may take weeks to recover from. Research consistently points to a set of principles that make exercise therapy effective for managing POTS:
| Principle | Why It Matters for POTS |
| Individualization | POTS presents differently in every patient. Programs must be tailored to individual heart rate zones, symptom triggers, and current fitness level — not pulled from generic plans. |
| Progressive overload | Gradual increases in duration and intensity allow the cardiovascular and autonomic systems to adapt without triggering crashes or flares. |
| Heart rate monitoring | Exercising within safe heart rate zones is critical. A chest-strap heart rate monitor helps patients stay within their prescribed training zones and avoid dangerous spikes. |
| Recumbent-to-upright progression | Beginning horizontal and slowly moving toward upright positions mirrors how the nervous system adapts, reducing symptom risk at each stage. |
| Strength + cardio integration | Both modalities address different but complementary physiological deficits in POTS. Neither alone is sufficient for full symptom management. |
| Supervised training | Studies show supervised programs produce better outcomes and fewer setbacks than unsupervised exercise in POTS populations, particularly in the early stages. |
| Consistency over time | Short-term training (3 months) often produces improvement but may be insufficient for long-term changes. Life-long habits of regular activity are the ultimate goal. |
Common Exercise Mistakes POTS Patients Should Avoid
Many POTS patients start an exercise program with the best intentions but stumble on predictable pitfalls. Understanding these common mistakes can make a real difference in outcomes:
- Starting with upright cardio too soon: Running or standing elliptical before building a recumbent base typically triggers symptom flares and discourages continuation.
- Skipping warm-ups and cool-downs: These are non-negotiable for POTS patients. Abruptly stopping exercise can cause heart rate and blood pressure instability. Always taper in and out of effort.
- Ignoring hydration and salt intake: Adequate fluid and sodium intake before and during exercise helps maintain blood volume and reduce symptom severity. This pairs directly with exercise therapy.
- Pushing through symptom flares: POTS symptoms during exercise are signals, not weakness. Exercising through dizziness, severe fatigue, or chest discomfort can cause setbacks. Listening to the body is essential.
- Following generic fitness plans: Standard coaching programs or popular cardio plans are not designed for autonomic dysfunction. Without expert guidance, they often do more harm than good.
The Long Game: Why Consistency Is Non-Negotiable
One of the most important — and often overlooked — findings in POTS exercise research is that short-term training is rarely enough for lasting change. Research from UT Southwestern Medical Center found that while three months of training improved cardiovascular function in POTS patients, the improvements were not fully sustained without continued effort. Longer training durations are needed to fundamentally reverse the deconditioning cycle and produce meaningful quality-of-life changes.
This makes consistency not just a fitness goal but a medical necessity. Life-long regular physical activity — ideally at least 4 to 5 sessions per week as tolerated — is associated with profound improvements in cardiovascular structure and autonomic control in POTS patients. The key is building habits that are sustainable, enjoyable, and adapted to the realities of living with a fluctuating condition.
Progress in POTS is rarely linear. There will be good weeks and harder ones. The most important thing is to have a structured plan that accounts for that variability and a support system — whether medical, personal, or professional — that helps you stay on track without pushing you into harmful territory.
| WORK WITH A SPECIALIST
Ready to Train Smarter With POTS? At Redefine Fitness, our certified trainers specialize in working with individuals living with POTS and other autonomic conditions. We build personalized, progressive programs that meet you where you are — safely and effectively. |
How Redefine Fitness Trainers Can Help POTS Patients
Managing POTS through exercise is a science — and it requires a guide who understands both the condition and the body. At Redefine Fitness (redefine-fitness.com), our trainers work with clients who live with POTS, dysautonomia, and related chronic conditions, designing evidence-informed programs that respect the unique demands of each individual’s health status.
Our approach for POTS clients is built on the same principles validated in clinical research:
- Comprehensive initial assessment of your current fitness level, symptom patterns, and personal goals
- Progressive programs that begin in recumbent or seated positions and advance at a pace your body can handle
- Integration of strength training and cardiovascular work tailored to your POTS stage and tolerance
- Ongoing monitoring, adjustment, and accountability to keep you moving forward safely
- Coordination with your medical team to ensure your exercise plan aligns with your broader treatment strategy
You deserve a fitness experience that sees the full picture of your health — not just a generic program handed to you without context. Our team is here to be that partner on your journey.
Sources & References
- Dani Brum et al. (2024). Exercise in Postural Orthostatic Tachycardia Syndrome: Focus on Individualized Exercise Approach. Journal of Clinical Medicine, 13(22), 6747.
- Fu Q & Levine BD. (2018). Exercise and Non-Pharmacological Treatment of POTS. PMC / Autonomic Neuroscience. pmc.ncbi.nlm.nih.gov/articles/PMC6289756/
- Shibata S et al. (2015). Exercise in the Postural Orthostatic Tachycardia Syndrome. PMC / Autonomic Neuroscience. pmc.ncbi.nlm.nih.gov/articles/PMC4336603/
- Multiple Authors. (2024). Exercise Interventions in the Management of POTS: A Scoping Review. PMC. pmc.ncbi.nlm.nih.gov/articles/PMC11646465/
- Children’s Hospital of Philadelphia. CHOP Modified Dallas POTS Exercise Program. Dysautonomia International.
- Le et al. (2024). POTS Global Training Guidelines for Cardio. Oregon Health & Science University.
- Hope Brain & Body Recovery Center. (2024). Effective Exercises for POTS: A Comprehensive Guide. hopebraincenter.com
- Shibata S, Fu Q, Bivens TB, Hastings JL, Wang W, Levine BD. (2012). Short-term exercise training improves the cardiovascular response to exercise in the postural orthostatic tachycardia syndrome. J Physiol. PMC3547265.