Osteoarthritis is one of the most common reasons adults on Long Island slow down. It starts quietly: a knee that complains on stairs, a hip that stiffens after sitting, a walk that gets shorter each season. The instinct is to protect the joint by moving it less. Decades of exercise science point the other way. Structured strength training, dosed correctly, is one of the most useful things you can do for a knee or hip affected by arthritis. This guide explains why, using the same training science we teach in our New York State approved Fitness Instructor apprenticeship curriculum, translated for anyone who wants to keep moving.
Why “Just Rest It” Fails Arthritic Joints
Our curriculum is blunt on this point: synovial joints benefit from movement, so full rest is not what they need. The knee and hip are synovial joints, which means they are lubricated by synovial fluid inside a joint capsule. Movement circulates that fluid. Long periods of rest do the opposite, and in an arthritic hip the capsule itself can lose fluid and constrict the joint further.
Rest also triggers a training principle called reversibility: progress begins to regress if it is not purposefully maintained. Muscle that took months to build starts fading within weeks of inactivity. For an arthritic joint this matters more, not less, because the surrounding muscle is doing extra work to protect it. Resting the joint quietly weakens the very system that supports it.
The honest caveat, straight from our curriculum: if a joint is producing very loud bone on bone symptoms, aggressive loading is not the answer, and that situation belongs in front of your physician first.
What Is Happening Inside the Joint
Arthritis in a joint involves a wearing down of the cartilage inside it. In the hip, the joint capsule typically loses synovial fluid as well, which constricts the joint and can allow grinding. In practice, people notice stiffness and reduced mobility, grinding sensations or sounds, discomfort aggravated by cold or unaccustomed exercise, and swelling during flare ups. Only your physician can diagnose arthritis or stage its severity. What we can explain is the mechanical context, because it shapes how training should look.
The knee is a hinge joint, like the elbow. Its distinctive feature is the patella, a floating bone held in place by the quadriceps and patellar tendon, which is why the health of the quadriceps has so much to say about how the front of the knee feels. Almost all of the work of bending and straightening the knee is done by two muscle groups: the quadriceps and the hamstrings.
The hip is a ball and socket joint, built like the shoulder but reinforced to carry the weight of the entire upper body. The bones are thicker, the connective tissue is stronger, and every joint action at the hip is performed by four or more large muscles: flexors, extensors, adductors, abductors, and rotators. Our curriculum puts it simply: strong and capable hips are often the difference between losing independence and staying active for decades.
Strong Muscles Are the Joint’s Support System
This anatomy leads to the core strategy for arthritic knees and hips, and it comes directly from our curriculum: strengthen the muscles surrounding the joint without excessive load or impact on the joint itself, stretch every muscle group that crosses it, and use soft tissue work such as myofascial release on the muscles around it.
For the knee, that means the quadriceps, hamstrings, calves, and the adductors and abductors of the hip. For the hip, it means restoring mobility across every joint action, then strengthening the surrounding musculature while avoiding impact and sharp pain. Muscle acts as the joint’s suspension system. The stronger and better conditioned the muscles that cross a joint, the less raw force the joint surfaces absorb on every step, squat, and stair.
The Training Principles That Make It Work
A joint-friendly program is not a random collection of gentle exercises. It is built on the same foundational principles as any well-designed program. Five matter most here.
Individuality. No two people respond to the same stimulus in the same way. Two clients with the same diagnosis on paper can need very different programs, which is why assessment comes before exercise selection.
Specificity. The body makes specific adaptations to specific stressors, a principle known as SAID: specific adaptations to imposed demands. If the goal is confident stairs, sit to stand strength, and stable walking, training must load those patterns, at tolerable intensities, rather than avoiding them forever.
Progressive overload. Stressors must increase over time for adaptations to continue. The levers are described by the FITT principle: frequency, intensity, time, and type. With an arthritic joint, we simply choose gentler levers first, nudging frequency or time before intensity, and choosing joint-friendly types of loading.
General adaptation syndrome. The body adapts to stress in phases. A training session temporarily drops performance below baseline. Recovery then raises it above baseline, an effect often called supercompensation. Push too hard for too long without recovery and the body enters an exhaustion phase: overtraining, lingering soreness, lost progress, and higher injury risk. Around an irritable joint, the job is to induce enough stress to adapt without tipping into that third phase.
Diminishing returns and reversibility. Progress slows as you advance, and it fades if it is not maintained. Both principles argue for consistency over intensity, which is exactly what most arthritic joints tolerate best.
What a Joint-Friendly Strength Session Looks Like
Structure does a lot of the protective work. Here is the session architecture we use, and why each piece is there.
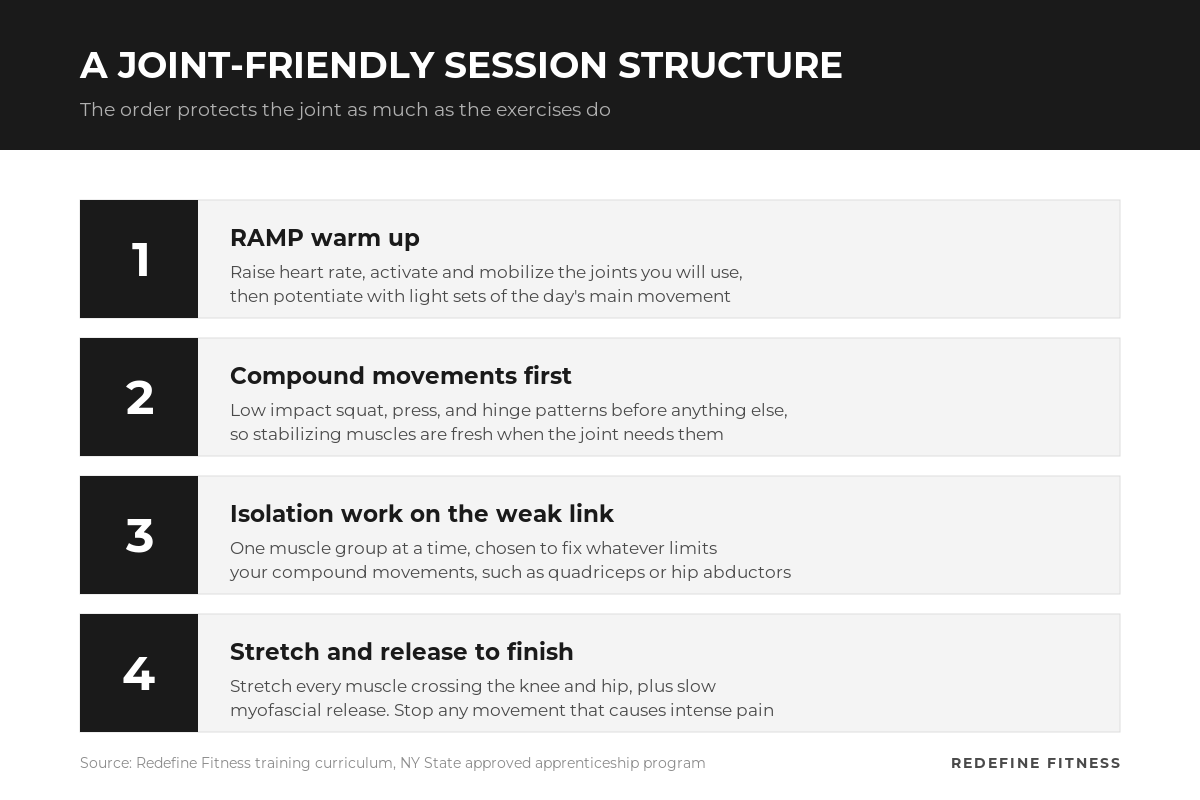
1. A RAMP warm up. Raise, activate and mobilize, potentiate. A few minutes of light cardio to raise heart rate, dynamic movement and myofascial release to activate and mobilize the joints and muscles you are about to use, then one or two light sets of the day’s main movement to potentiate it. Before a session, active range of motion work is preferred over long passive stretching, which can take muscles past their typical range and raise injury risk during the workout.
2. Compound movements first. Compound exercises use multiple muscle groups at once: lower body pushing patterns such as squat variations or the leg press, and lower body pulling patterns such as hip thrusts or hinge variations. They come first to avoid pre-exhausting the smaller muscles that stabilize and assist them, which protects both performance and the joint. For arthritic knees and hips, we bias toward low impact versions of these patterns and control the depth and load.
3. Isolation work that targets the weak link. Isolation exercises train one muscle group at a time and should be chosen to improve your compound movements. If the quadriceps are the limiting factor in a sit to stand, they get the isolation work. If the hip abductors are letting the knee drift inward, they do.
4. Stretching and soft tissue work to finish. Restricted range of motion forces the body into compensation patterns, and those inefficient patterns often feed joint irritation. Slow, steady pressure through foam rolling or similar myofascial release improves local blood flow and tissue pliability and can reduce pain signaling.
A note on honesty: our curriculum does not prescribe fixed set and rep formulas for arthritis, because dosage is individual. As general best practice, not curriculum doctrine, most people do well starting with two or three strength sessions per week on nonconsecutive days, and many find isometric holds comfortable on days when a joint is irritable. Your program should be built around your response, not a template.
How to Progress Without Flaring Up
Progression around an arthritic joint is a judgment skill, and it is one of the main things a supervised program buys you. We watch objective cues. If the lifting phase of a movement is fast and crisp, it is time to progress. If it grinds on far too long, or the muscles begin to shake, it is time to regress. We also respect a simple rule that appears throughout our curriculum: stop if there is intense pain. Pushing through sharp pain is how training problems become injuries.
Progression must also match the goal. A powerlifter progresses strength, an athlete progresses explosiveness, and for many older adults the priority is stability. For an arthritic knee or hip, progress usually means more confident movement at gradually increasing loads, not maximal numbers.
Why Assessment Comes First
Because individuality is the first principle, every program should start with an assessment, not a workout. For knees, our curriculum starts at the feet, since collapsing arches and overpronation often present as knee problems. We then look at tibiofemoral alignment, checking whether the kneecaps face inward, forward, or outward, and at how the patella tracks as the knee bends and straightens. For hips, structured tests such as the Thomas test for tight hip flexors and the FABER test help map which tissues are restricted before any load is applied.
This is the difference between a medical-fitness program and a generic workout plan. In our private 1-on-1 sessions, a Fitness Specialist builds the program around what your body actually shows us, done with you, at a done for you standard.
Training Alongside Your Care Team
Strength training for an arthritic joint is not a replacement for medical care. It works alongside it. Your physician diagnoses and manages the condition. If you have been through physical therapy, we pick up where discharge left off, keeping the momentum your therapist built. Bring us your provider’s guidance and restrictions, and we will program within them. If you are returning to exercise after surgery or a long layoff, our guide to exercising with joint pain and after joint surgery covers that transition in detail.
Move Better, With a Plan Built for Your Joints
Arthritic knees and hips do not need less movement. They need better movement: assessed first, loaded intelligently, progressed patiently, and coordinated with your care team. That is what we build every day at our Mount Sinai studio at 271 Route 25A and our Stony Brook studio at 1113 North Country Road.
If a knee or hip has been shrinking your life, start with a conversation. Book Your Complimentary Consultation and we will map out what a joint-friendly program looks like for you.